Interpreting Iron Studies
Iron studies are one of the most commonly ordered laboratory tests.
The figure below shows a schematic representation of the few common laboratory tests
of iron balance,
and how they relate to iron storage and transport.
The figure below shows a schematic representation of the few common laboratory tests
of iron balance,
and how they relate to iron storage and transport.
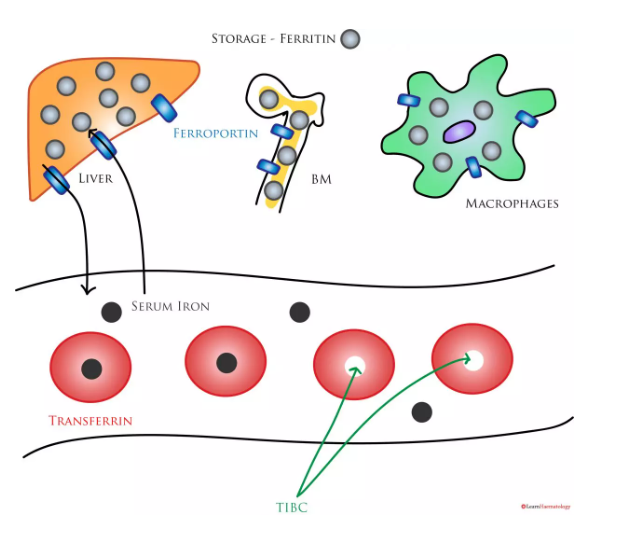
Laboratory Measures of Iron Balance
.
Ferroportin Transport Channels:
Iron enters and exits the storage compartments via ferroportin (blue rectangle).
Ferritin Protein
(light grey circle) is the main storage protein.
Serum iron
is a measure of circulating iron,(bound AND unbound) most of which is bound to transferrin.
Transferrin Protein
: THE BLOOD TRANSPORT PROTEINIRON in the blood
- may be free (black circle),
- or bound to transferrin (red balls).
(do not confuse for red blood cells)
Total(Transferrin protein) Iron Binding Capacity (TIBC)
is the amount of available iron binding sites ON THE TRANSFERRIN Proteins. Transferrin Saturation
is calculated by dividing the serum iron by the TIBC.(serum Iron (both bound and unbound)
devided by Transferrin proteins which are ?not or ? not yet, carrying any iron for some reason
The serum iron level is low in iron deficiency and inflammatory anaemia
because it depends on efficient recycling of iron through macrophages and the bone marrow.
In iron deficiency, there is insufficient iron for iron recycling,
While in inflammatory anaemia,
increased hepcidin levels result in iron trapping in macrophages.
Transferrin
is the main iron transport protein;
its synthesis is inversely proportional to body iron stores.
Hence, levels increase in iron deficiency to facilitate iron absorption.
Transferrin levels are often low in inflammatory anaemia
as transferrin expression is negatively affected by cytokines.
Ferritin
is the main iron storage protein. The normal range is 15 – 300 µg/dL.
The sensitivity and specificity of the test vary
depending on cut-off levels used to define iron deficiency;
At a cut-off level of 15µg/L,
the test is highly specific for iron deficiency, but lacks sensitivity.
At a cur-off level of 100µg/L,
the sensitivity increases to 94%,
at the expense of specificity (71%).
Ferritin is a positive acute phase reactant;
levels increase in inflammation.
In addition,
levels in inflammatory anaemia may also be high
because of
ferritin secretion by iron-retaining macrophages.
The total iron binding capacity (TIBC)
reflects the available iron binding sites on transferrin. It requires the measurement of serum iron and transferrin that is not bound to iron
(i.e., the unbound iron binding capacity, UIBC).
The TIBC is the sum of serum iron (black dots) and the UIBC (empty red balls)
TIBC and transferrin are essentially different measures of the same parameter.
The TIBC is high in iron deficiency
The TIBC is low in inflammatory anaemia.
The transferrin saturation
is the ratio of serum iron to the TIBC,expressed as a percentage.
Levels fall in both iron deficiency and inflammatory anaemia.
The table below summarises the changes in the various laboratory indicies in different disease states:
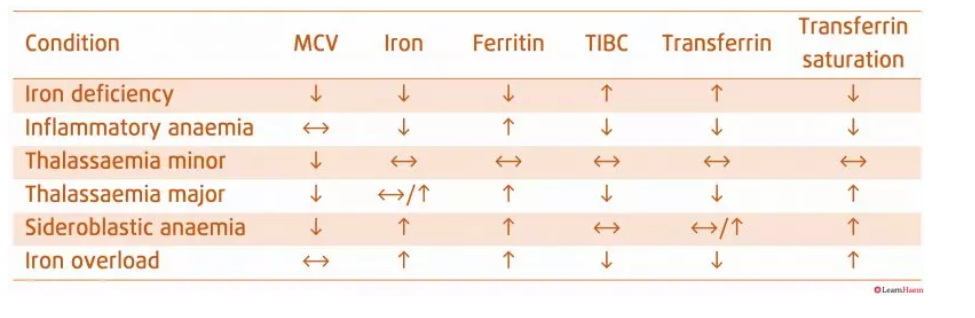
Iron Indices.
Ferritin is the most specific marker of iron deficiency;
its sensitivity is dependent on the cut-off value.
A serum ferritin of <30µ/L is very sensitive for iron deficiency.
Ferritin is the most specific marker of iron deficiency;
its sensitivity is dependent on the cut-off value.
A serum ferritin of <30µ/L is very sensitive for iron deficiency.