.png)

Assessing the axis on an ECG
Axis is the sum of all the electrical activity in the heart.
The contraction travels from the atria to the ventricular septum and then to both ventricles.
As the left ventricle is larger and more muscular
normal axis lies to the left (at -30 degrees to 90 degrees.)
i.e lead 2
The contraction travels from the atria to the ventricular septum and then to both ventricles.
As the left ventricle is larger and more muscular
normal axis lies to the left (at -30 degrees to 90 degrees.)
i.e lead 2
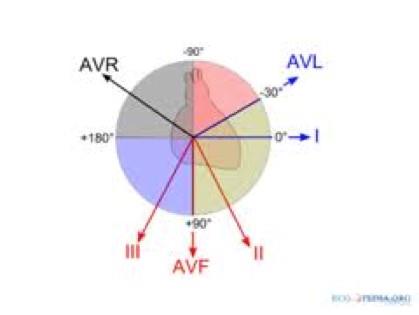
If lead I has a positive deflection
and aVF has a negative deflection
then there is left axis deviation
and aVF has a negative deflection
then there is left axis deviation
If lead I has a net negative deflection
whilst aVF is positive
then there is right axis deviation
whilst aVF is positive
then there is right axis deviation
If the net deflections in leads I and aVF are positive
then the axis is normal.
then the axis is normal.
6. P-wave and PR interval
Can you see a p-wave?
If the rhythm is atrial fibrillation, atrial flutter or a junctional tachycardia you may not be able to.
P:QRS Ratio
At this point you can also assess whether each p wave is associated with a QRS complex.
P-waves not in association with QRS complexes indicate complete heart block.
Assess p-wave morphology
The PR interval
A notched (or bifid) p-wave known as
“p mitrale”,
indicative of left atrial hypertrophy
which may be caused by Mitral stenosis
“p mitrale”,
indicative of left atrial hypertrophy
which may be caused by Mitral stenosis
|
|


Pathological Q-waves
|
|
|
|
|
|
|
|
The QRS may be small
(or low voltage) in
- high BMI,
- emphysema,
- pericardial effusion,
- cardiomyopathy
- cardiac amyloid.
(or low voltage) in
- high BMI,
- emphysema,
- pericardial effusion,
- cardiomyopathy
- cardiac amyloid.
The QRS is tall in left ventricular hypertrophy (LVH)
The criteria suggestive of LVH on the ECG
is if the height of the R wave in V6
+ the depth of the S wave in V1.
If this value is >35mm
this is suggestive of LVH.
The criteria suggestive of LVH on the ECG
is if the height of the R wave in V6
+ the depth of the S wave in V1.
If this value is >35mm
this is suggestive of LVH.


ST depression
is normally due to ischaemia
Look out for reciprocal changes.
ST segment depression
may also be seen in digoxin toxicity.
Here the ST depression will be downsloping
(sometimes known as the
“ST reverse tick” sign).
is normally due to ischaemia
.
Look out for reciprocal changes.
ST segment depression
may also be seen in digoxin toxicity.
Here the ST depression will be downsloping
(sometimes known as the
“ST reverse tick” sign).
|
|
|
9. QT interval
The QT interval is the time between the start of the q-wave and the end of the t-wave.
The QT interval is corrected for heart rate giving the QTc.
The QT interval is corrected for heart rate giving the QTc.
As a quick check, if the t-waves occur over half way between the QRS complexes
the QTc may be lengthened
Not an accurate method but very quick!
A long QTc interval (known as “long QT”)
is especially important to identify
in patients with a history of collapse
or transient loss of consciousness.
the QTc may be lengthened
Not an accurate method but very quick!
A long QTc interval (known as “long QT”)
is especially important to identify
in patients with a history of collapse
or transient loss of consciousness.
Drugs |
Metabolic |
Familial |
Other |
Erythromycin Amiodarone Tricyclic antidepressants (TCAs) Terfenadine Phenothiazines Quinidine |
Hypothermia Hypothyroidism Hypokalaemia Hypocalcaemia
|
Long QT syndrome Brugada syndrome Arrhythmogenic RV dysplasia |
IHD Myocarditis |
Causes of long QT:


ST elevation
indicates infarction.
indicates infarction.