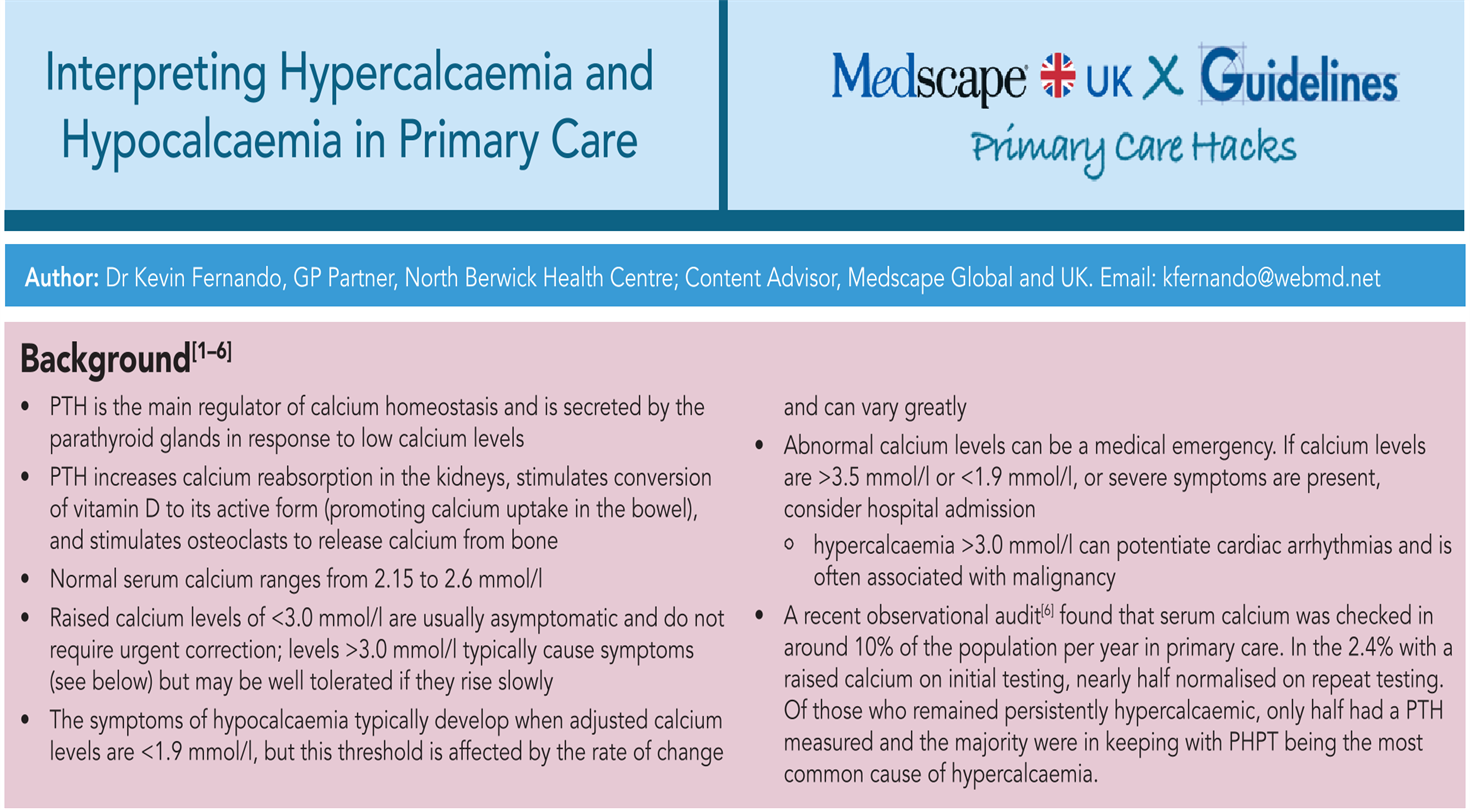
MEDSCAPE GP HACKS
.png)