.png)
MAGNESIUM
Magnesium is an essential component of soft tissues and bone.
It is required for the normal functioning of muscle and nervous tissue.
It exerts effects similar to those of calcium
and acts directly at the motor endplate.
It is an important activator ion
participating in the function of many enzymes involved in phosphate transfer reactions.
Bone:
50% of the total
insoluble
Cells:
45% of the total
a cation required as a co-factor for ATP, etc.
Extracellular fluid:
5% of the total
It is abundant in the normal diet and is eliminated in the urine and faeces.
Note that reference ranges may vary between different laboratories
Changes in plasma magnesium usually induce changes in calcium.
Hypomagnesaemia impairs PTH secretion
and may also impair end organ response to PTH.
It is required for the normal functioning of muscle and nervous tissue.
It exerts effects similar to those of calcium
and acts directly at the motor endplate.
It is an important activator ion
participating in the function of many enzymes involved in phosphate transfer reactions.
Magnesium is found in:
Bone:
50% of the total
insoluble
Cells:
45% of the total
a cation required as a co-factor for ATP, etc.
Extracellular fluid:
5% of the total
The normal plasma range is 0.75 to 1.0 mmol/l.
It is abundant in the normal diet and is eliminated in the urine and faeces.
Note that reference ranges may vary between different laboratories
Magnesium and Calcium
Changes in plasma magnesium usually induce changes in calcium.
Hypomagnesaemia impairs PTH secretion
and may also impair end organ response to PTH.

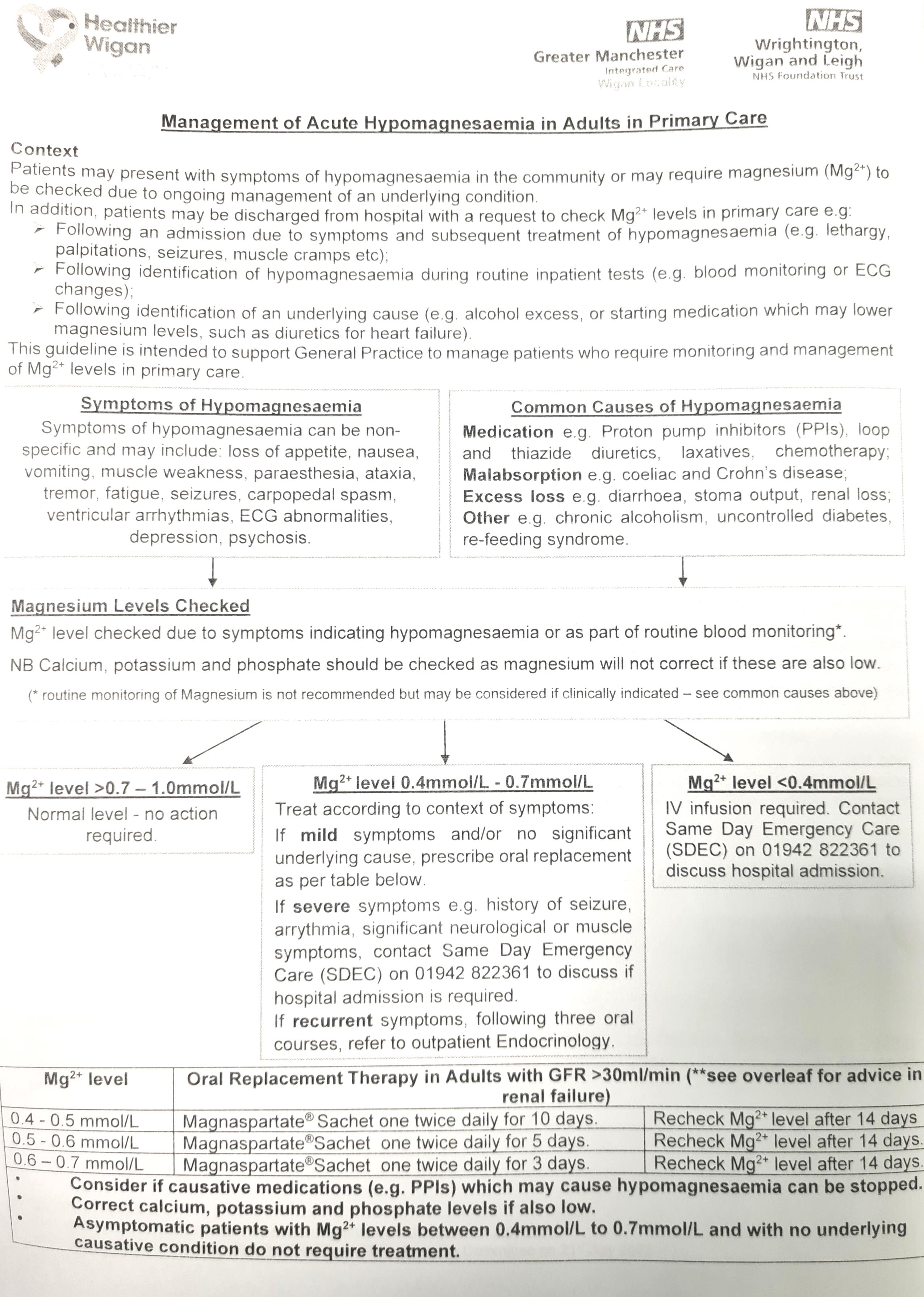
Magnesium deficiency
Magnesium deficiency can result in
1. Symptoms similar to those of hypocalcaemia
- Irritability, aggression
- Muscle twitching,
- Tetany,
- Convulsions
- Magnesium deficiency may cause ventricular arrhythmias
such as torsade de pointes
2. Signs of
- Nystagmus,
- Athetoid movements,
- Babinski positive response.
Acute magnesium deficiency Treatment
Magnesium is given intravenously, usually as chloride or sulphate
serum levels must be monitored so as to prevent levels from rising above 2.5 mmol/l
potassium and calcium supplementation may be required
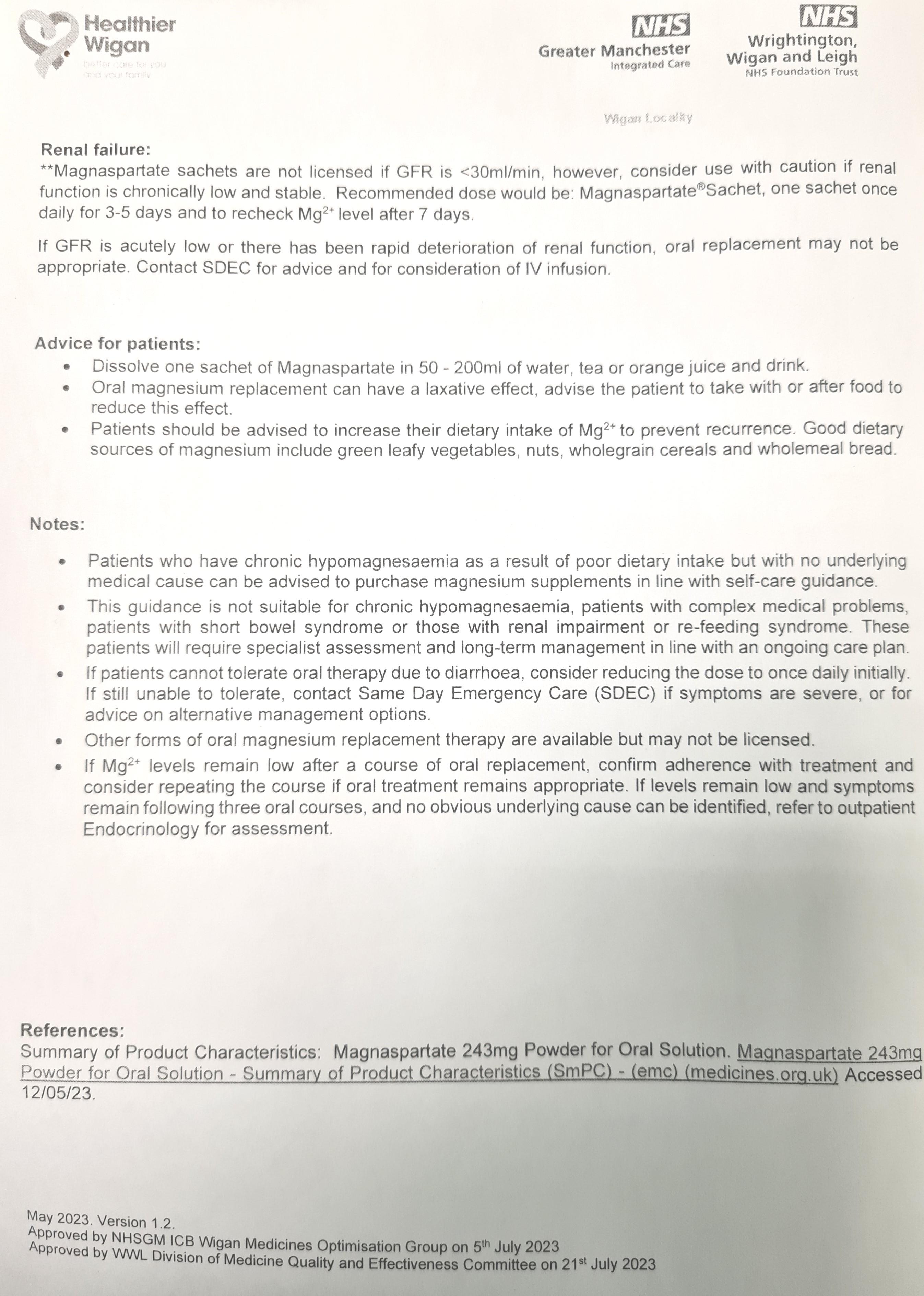
Chronic magnesium deficiency Treatment
Chronic hypomagnesaemia may be treated using
magnesium oxide, 250-500 mg, by mouth, 2-4 times daily
The administration of calcium is ineffective.
Causes of magnesium deficiency include:
low uptake:
- rare because magnesium is ubiquitous
- Kwashiorkor
- severe alcholism
- malabsorption
- parenteral nutrition without adequate Mg++
increased loss:
- diabetic ketoacidosis
- steatorrhea
- inflammatory bowel disease: Crohn's > ulcerative colitis
- prolonged vomiting
- hyperaldosteronism
- mannitol-induced diuresis
miscellaneous:
- excess vitamin D therapy
- hyperparathyroidism
- postparathyroidectomy
- drugs e.g. cisplatin, gentamicin
Magnesium excess
Hypermagneaemia is predominantly the result of renal failure.
Occasionally, it occurs
- when magnesium salts are given rectally in patients with colonic disease
- or in association with hypothyroidism, lithium therapy and the milk alkali syndrome.
Symptoms of hypermagnesaemia are usually apparent at levels above 2 mmol/l.
Features of magnesium excess include:
- muscle weakness - with possibly, a flaccid paralysis
- confusion and mental obtundation
- respiratory paralysis
- cardiac arrest - in extreme cases
The ECG may show increased PR interval, broadened QRS complex or elevated T waves.
Treatment is directed at the underlying cause.
Calcium chloride may be given intravenously as it is antagonistic to magnesium;
500 mg or more at a rate of 100 mg/min is typical.
Haemodialysis or peritoneal dialysis may be indicated in acute renal failure.
