
Clinical implications and rationale
Adverse patient outcomes associated with AKI are not limited to episodes of acute illness
with many patients remaining at risk of poor outcomes following AKI.
These include:
Increased risk of unplanned 90-day hospital readmission
highlighting a need to coordinate timely post-AKI care across the secondary-primary care interface
Increased risk of new or worsening chronic kidney disease (CKD)
Increased risk of cardiovascular disease (especially if CKD 3B, 4 or 5 are present)
Increased short and longer-term mortality
Key elements of Post-AKI care
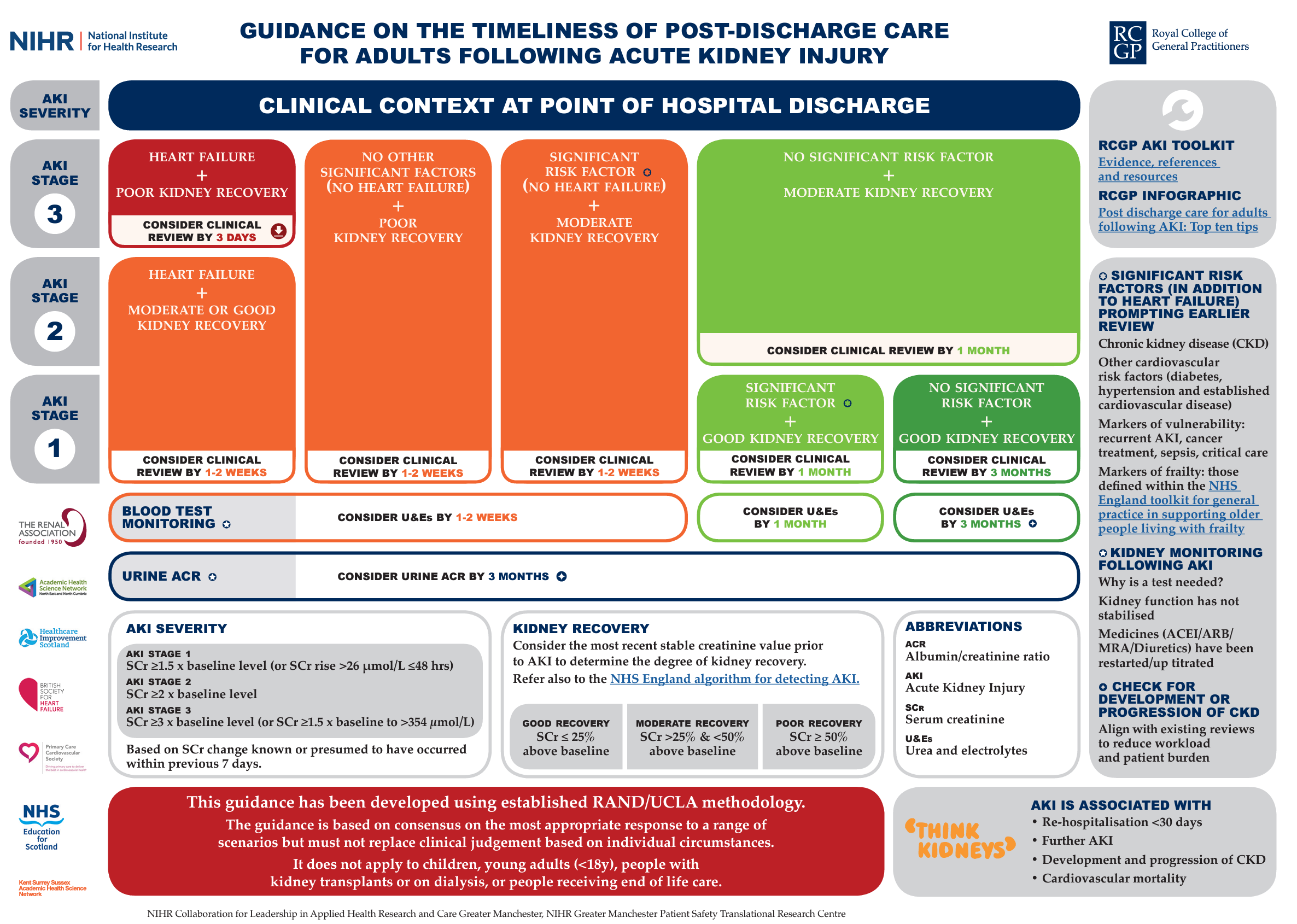
Post-AKI care should be personalised to consider existing co-morbidities
as AKI is a clinical syndrome with various causes and variable adverse outcomes,
affecting a heterogeneous patient population.
Factors determining the urgency of review include the cause(s) of the AKI, its severity, and the degree of kidney recovery following AKI.
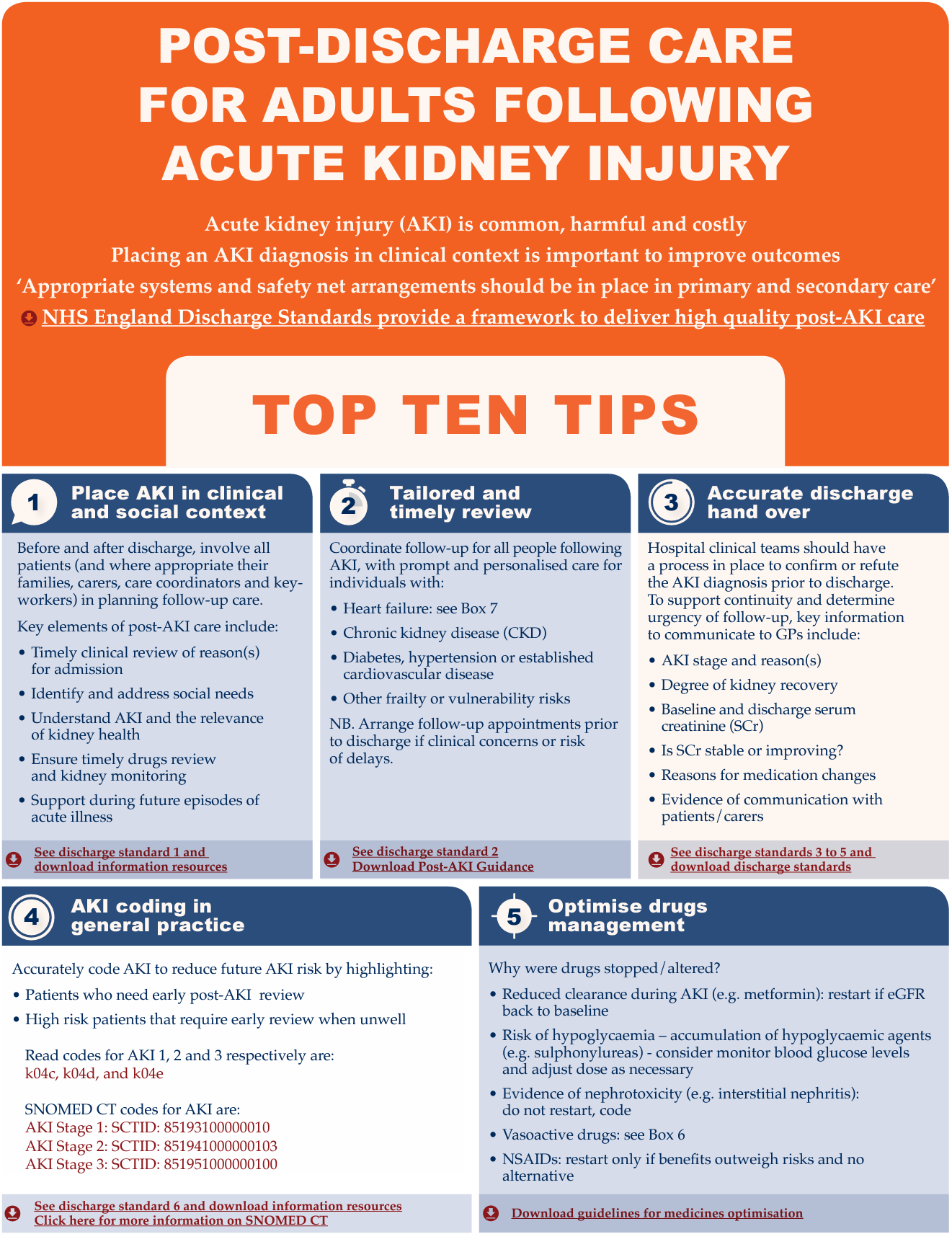
Key elements of post-AKI care include:
Ensuring accurate diagnostic coding of AKI
Optimising medicines management
Coordinating monitoring of kidney function
Communicating kidney health and AKI risk with patients and carers
Ensuring accurate diagnostic coding of AKI
NICE has recommended that primary care teams establish AKI patient registers to facilitate systematic care for this high risk patient population. These aim to help:
Identify patients that require timely post-AKI care planning
Highlight vulnerable patients that require prompt review when acutely unwell
Support quality assurance and future QI interventions
Optimising medicines management
Optimising medicines management underpins safe post-AKI care.
Key questions to consider include:
Medication review post-AKI
Have medicines been stopped during the episode of acute illness?
What were the original indications for these medications?
Are there strong prognostic indications to restart medications?
If, when, and how should medications be restarted?
What is the patient’s blood pressure?
Should any medications (e.g. NSAIDs) be discontinued?
Is there an opportunity to rationalise medications and avoid unnecessary polypharmacy?
It is really important to restart drugs with prognostic benefit following AKI,
as a failure to do so can result in avoidable patient harm.
Timely reconciliation of medications post-AKI, tailored to a patient’s acute and chronic co-morbidities,
will mitigate such adverse outcomes -
Patients with chronic heart failure represent a common exemplar patient group.
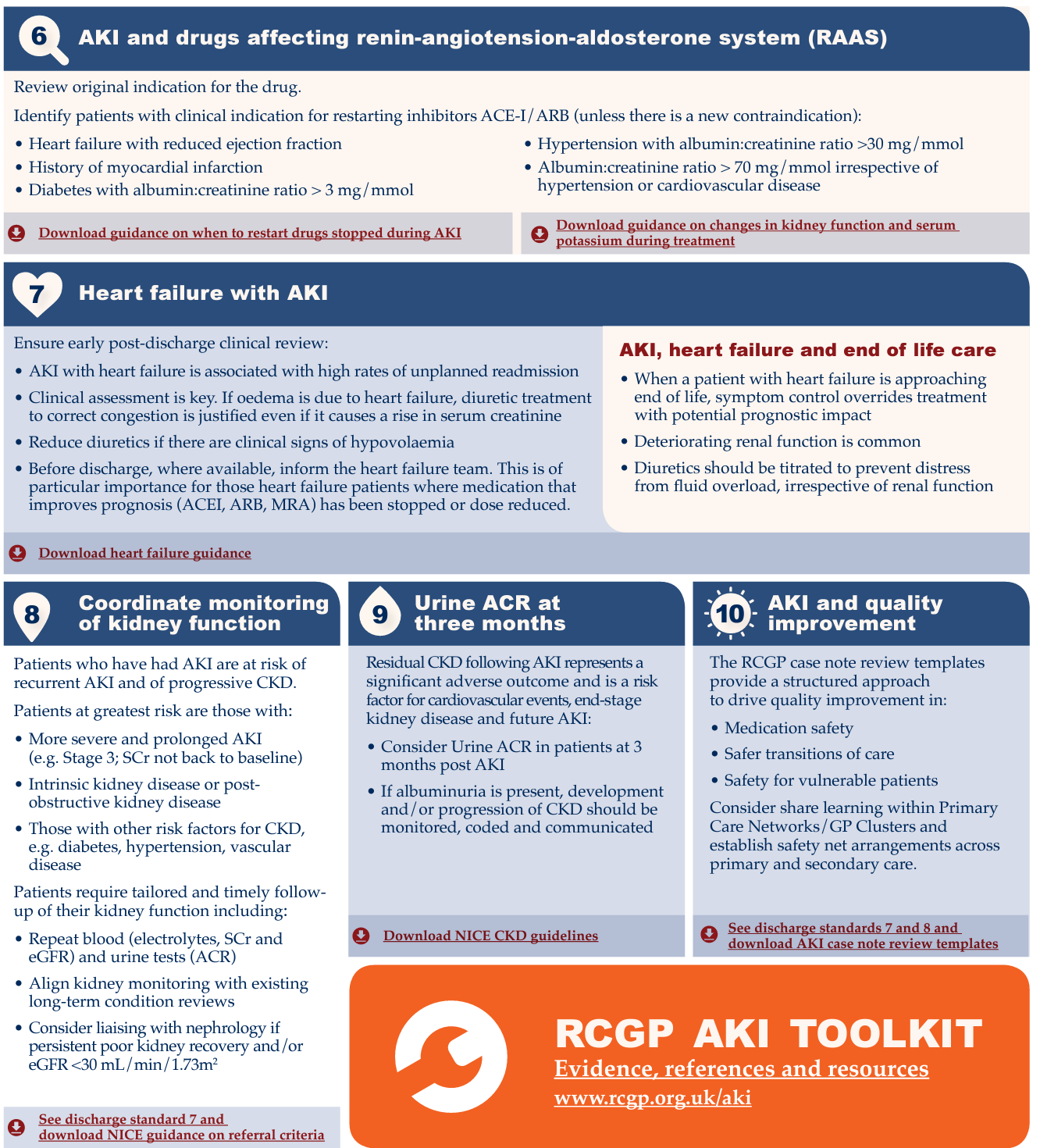
While it is sometimes appropriate to "withhold" ACE-inhibitors and diuretic drugs during AKI episodes,
patients with chronic heart failure are at high risk of decompensated heart failure,
hospital readmission and death if these drugs are not reviewed post-AKI.
Medication review post-AKI may also provide opportunities to:
Minimise polypharmacy - Polypharmacy guidance (NHS Scotland) provides a stepwise approach to support decision making with patients living with complex health and social care needs (e.g. patients living with dementia; end of life care)
Stop (or restrict) the use of NSAIDS unless there is a ‘compelling need.’
Coordinating monitoring of kidney function
Patients who have sustained AKI are at increased risk of developing new or worsening chronic kidney disease (CKD),
even when they have recovered from AKI.
Residual CKD following AKI represents a significant adverse outcome, and is a risk factor for cardiovascular, end-stage kidney disease and further AKI.
Risk of developing new or worsening CKD is higher if:
- Kidney function remains below pre-AKI baseline
- AKI is severe or there are repeated AKI episodes
- There are risk factors for CKD (eg. diabetes mellitus)
International consensus guidance recommends evaluating a patient’s kidney function 3 months after an episode of AKI
to check for new onset, worsening or pre-existing CKD.
Earlier monitoring should be prioritised if serum creatinine has not returned to a patient’s pre-AKI baseline,
or if stipulated at point of hospital discharge.
Non-recovery of kidney function 3 months post-AKI usually indicates new or worsening CKD
and frequency of onward monitoring should follow NICE CKD guidance.
Where appropriate, assessment of a patient’s kidney health should include
blood tests (electrolytes, serum creatinine and eGFR) to check for kidney function
and a urine test (I.e. urinary albumin:creatinine ratio, ACR) to assess for evidence of proteinuria.
AKI Care in context
In the context of providing person-centred care, kidney function monitoring needs to be tailored
to a patient's individual health and social care needs.
Key questions to consider include:
What is the overall clinical context?
Do not treat the test result in isolation;
trade-offs may be required in the management of patients with heart failure, for example.
Are there co-morbidities strongly associated with adverse outcomes (CKD, heart failure, diabetes)?
Follow-up should be prioritised regardless of the degree of renal recovery.
Has the episode of AKI been coded and communicated with the patient?
Has the CKD been coded and communicated with the patient?
Can follow-up prioritise person-centred care?
Aligning kidney monitoring with pre-existing routine long-term condition review appointments may reduce patient burden.
Communicating kidney health and AKI risk with patients and carers
Generating an agreed action plan with patients may help ensure timely review of medicines and kidney monitoring
as well as support management of future episodes of acute illness.
Patient and Carer education
‘If you are unwell and unable to drink properly, particularly if you are losing excess fluid through vomiting or diarrhoea, or you have a high temperature and sweats, then it is important that you discuss your condition with a medical professional. This may be your GP or a specialist nurse, e.g. a heart failure or kidney nurse if you have one. You may be advised to discontinue taking medications which lower your blood pressure for a short time and a blood test will be arranged to check your kidney function.
If you are admitted to hospital for a specialist x-ray or operation, you should make your health care team aware if you have Chronic Kidney Disease.
If you are only passing small amounts of urine you may need admission to hospital and you should alert your GP to this.’
RCGP safety netting Advice
Advising patients ‘when to worry’
Advising patients when to return for a review
Providing verbal and/or written information
Fixing follow-up before the patient leaves the consultation (when necessary)
Read coding and clear documentation
Sick day guidance: Advising selected patients about cessation of medicines during specific acute illnesses (“Sick Day Guidance”) may form part of proactive care planning post-AKI. This should be decided upon an individual basis - such policies have not been formally evaluated and may risk inappropriate / unsafe self-medication changes if loosely applied to all patients. A Sick Day Guidance Position Statement (Think Kidneys Programme Board) includes:
‘In terms of medicines management, advice from the Think Kidneys Programme Board is that it is reasonable for clinicians to provide sick day guidance on temporary cessation of medicines to patients deemed at high risk of AKI based on an individual risk assessment. However, we consider that investment in a systematic approach to increase uptake of sick day rules guidance by patients should only be undertaken in the context of a formal evaluation.’
Adverse patient outcomes associated with AKI are not limited to episodes of acute illness
with many patients remaining at risk of poor outcomes following AKI.
These include:
Increased risk of unplanned 90-day hospital readmission
highlighting a need to coordinate timely post-AKI care across the secondary-primary care interface
Increased risk of new or worsening chronic kidney disease (CKD)
Increased risk of cardiovascular disease (especially if CKD 3B, 4 or 5 are present)
Increased short and longer-term mortality
Key elements of Post-AKI care
Post-AKI care should be personalised to consider existing co-morbidities
as AKI is a clinical syndrome with various causes and variable adverse outcomes,
affecting a heterogeneous patient population.
Factors determining the urgency of review include the cause(s) of the AKI, its severity, and the degree of kidney recovery following AKI.
Key elements of post-AKI care include:
Ensuring accurate diagnostic coding of AKI
Optimising medicines management
Coordinating monitoring of kidney function
Communicating kidney health and AKI risk with patients and carers
Ensuring accurate diagnostic coding of AKI
NICE has recommended that primary care teams establish AKI patient registers to facilitate systematic care for this high risk patient population. These aim to help:
Identify patients that require timely post-AKI care planning
Highlight vulnerable patients that require prompt review when acutely unwell
Support quality assurance and future QI interventions
Optimising medicines management
Optimising medicines management underpins safe post-AKI care.
Key questions to consider include:
Medication review post-AKI
Have medicines been stopped during the episode of acute illness?
What were the original indications for these medications?
Are there strong prognostic indications to restart medications?
If, when, and how should medications be restarted?
What is the patient’s blood pressure?
Should any medications (e.g. NSAIDs) be discontinued?
Is there an opportunity to rationalise medications and avoid unnecessary polypharmacy?
It is really important to restart drugs with prognostic benefit following AKI,
as a failure to do so can result in avoidable patient harm.
Timely reconciliation of medications post-AKI, tailored to a patient’s acute and chronic co-morbidities,
will mitigate such adverse outcomes -
Patients with chronic heart failure represent a common exemplar patient group.
While it is sometimes appropriate to "withhold" ACE-inhibitors and diuretic drugs during AKI episodes,
patients with chronic heart failure are at high risk of decompensated heart failure,
hospital readmission and death if these drugs are not reviewed post-AKI.
Medication review post-AKI may also provide opportunities to:
Minimise polypharmacy - Polypharmacy guidance (NHS Scotland) provides a stepwise approach to support decision making with patients living with complex health and social care needs (e.g. patients living with dementia; end of life care)
Stop (or restrict) the use of NSAIDS unless there is a ‘compelling need.’
Coordinating monitoring of kidney function
Patients who have sustained AKI are at increased risk of developing new or worsening chronic kidney disease (CKD),
even when they have recovered from AKI.
Residual CKD following AKI represents a significant adverse outcome, and is a risk factor for cardiovascular, end-stage kidney disease and further AKI.
Risk of developing new or worsening CKD is higher if:
- Kidney function remains below pre-AKI baseline
- AKI is severe or there are repeated AKI episodes
- There are risk factors for CKD (eg. diabetes mellitus)
International consensus guidance recommends evaluating a patient’s kidney function 3 months after an episode of AKI
to check for new onset, worsening or pre-existing CKD.
Earlier monitoring should be prioritised if serum creatinine has not returned to a patient’s pre-AKI baseline,
or if stipulated at point of hospital discharge.
Non-recovery of kidney function 3 months post-AKI usually indicates new or worsening CKD
and frequency of onward monitoring should follow NICE CKD guidance.
Where appropriate, assessment of a patient’s kidney health should include
blood tests (electrolytes, serum creatinine and eGFR) to check for kidney function
and a urine test (I.e. urinary albumin:creatinine ratio, ACR) to assess for evidence of proteinuria.
AKI Care in context
In the context of providing person-centred care, kidney function monitoring needs to be tailored
to a patient's individual health and social care needs.
Key questions to consider include:
What is the overall clinical context?
Do not treat the test result in isolation;
trade-offs may be required in the management of patients with heart failure, for example.
Are there co-morbidities strongly associated with adverse outcomes (CKD, heart failure, diabetes)?
Follow-up should be prioritised regardless of the degree of renal recovery.
Has the episode of AKI been coded and communicated with the patient?
Has the CKD been coded and communicated with the patient?
Can follow-up prioritise person-centred care?
Aligning kidney monitoring with pre-existing routine long-term condition review appointments may reduce patient burden.
Communicating kidney health and AKI risk with patients and carers
Generating an agreed action plan with patients may help ensure timely review of medicines and kidney monitoring
as well as support management of future episodes of acute illness.
Patient and Carer education
‘If you are unwell and unable to drink properly, particularly if you are losing excess fluid through vomiting or diarrhoea, or you have a high temperature and sweats, then it is important that you discuss your condition with a medical professional. This may be your GP or a specialist nurse, e.g. a heart failure or kidney nurse if you have one. You may be advised to discontinue taking medications which lower your blood pressure for a short time and a blood test will be arranged to check your kidney function.
If you are admitted to hospital for a specialist x-ray or operation, you should make your health care team aware if you have Chronic Kidney Disease.
If you are only passing small amounts of urine you may need admission to hospital and you should alert your GP to this.’
RCGP safety netting Advice
Advising patients ‘when to worry’
Advising patients when to return for a review
Providing verbal and/or written information
Fixing follow-up before the patient leaves the consultation (when necessary)
Read coding and clear documentation
Sick day guidance: Advising selected patients about cessation of medicines during specific acute illnesses (“Sick Day Guidance”) may form part of proactive care planning post-AKI. This should be decided upon an individual basis - such policies have not been formally evaluated and may risk inappropriate / unsafe self-medication changes if loosely applied to all patients. A Sick Day Guidance Position Statement (Think Kidneys Programme Board) includes:
‘In terms of medicines management, advice from the Think Kidneys Programme Board is that it is reasonable for clinicians to provide sick day guidance on temporary cessation of medicines to patients deemed at high risk of AKI based on an individual risk assessment. However, we consider that investment in a systematic approach to increase uptake of sick day rules guidance by patients should only be undertaken in the context of a formal evaluation.’
Post-AKI Care: Primary care management after an episode of AKI
Informed by RAND/UCLA methodology, provides consensus guidance to support tailored and timely care
following a hospital admission complicated by acute kidney injury.
following a hospital admission complicated by acute kidney injury.
CLICK IMAGE FOR PDF AND CLICKABLE LINKS
CLICK IMAGE FOR PDF AND CLICKABLE LINKS
